.jpg "SHINING 3D DENTAL Logo")
Abstract
The prosthetic management of severe dental abrasion is a common yet challenging clinical issue in restorative dentistry. Long-term success depends on harmoniously integrating aesthetic, biological, functional, and mechanical parameters. Among these, occlusal considerations are paramount.
This report illustrates the comprehensive rehabilitation of a patient with advanced tooth wear, emphasising occlusal re-establishment and functional integration using the METISMILE® digital system.
Introduction
The rehabilitation of severe dental abrasion requires the restoration of both function and aesthetics, while ensuring long-term biomechanical stability. This equilibrium is achieved through a centred and stable static occlusion, an appropriate vertical dimension of occlusion (VDO), and an anterior guidance to protect the posterior teeth and temporomandibular joints during mandibular excursions. Taking the patient’s individual masticatory pattern into account further ensures physiological balance throughout treatment.
Clinical testing with provisional restorations is essential during the adaptation phase to enable dynamic functional validation prior to definitive restorations. Recent digital technologies, such as facial scanners, can record real-time masticatory dynamics, offering unprecedented precision and efficiency in occlusal and aesthetic design.
This report aims to demonstrate the clinical value of the METISMILE® system in the prosthetic rehabilitation of severe tooth wear, with a particular focus on re-establishing anterior guidance within a structured digital workflow.
Case Presentation
A 33-year-old male patient in good general health who was motivated yet time-constrained (treatment completed in five weeks) sought aesthetic improvement of his smile.
An extraoral examination revealed a hypertrophy of the elevator muscles with no other abnormalities present. The patient exhibited a gingival smile (Liebart Class I). The maxillary anterior teeth were not visible at rest and the patient had a reduced phonetic space producing whispered “S” sounds, indicating a collapsed VDO.




An intraoral assessment revealed moderate-to-severe tooth wear and an unaesthetic concave incisal plane. The periodontal tissues were healthy.
Although the primary complaint was aesthetic, functional re-establishment was considered the cornerstone of treatment.
The rehabilitation protocol consisted of three main phases :
- Acquisition of clinical and radiographic data
- Digital design of the prosthetic project
- Clinical implementation through provisional restorations
Phase 1: Clinical Data Acquisition
A new intermaxillary record was established in centric relation using a Lucia jig, with an increased VDO of +3mm. The occlusal relationship was digitized via the Aoralscan 3® intraoral scanner.
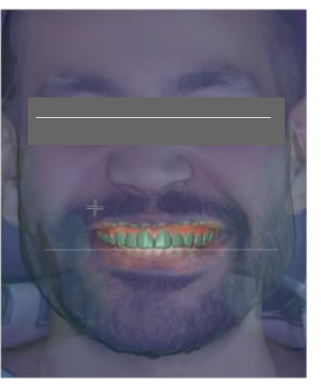
A 3D facial scan was performed using the METISMILE® system to generate a digital twin of the patient, replacing the traditional facebow. This enabled the dental arches to be optimized simultaneously for integration into the facial frame, midline alignment, and occlusal plane orientation relative to the facial reference planes. Digital analysis then refined the tooth proportions to improve morphologic harmony.


Beyond its esthetic contribution, the METISMILE® system offers a significant functional innovation. Using fluorescent markers on the maxillary and mandibular teeth, it records mandibular dynamics and converts the digital twin into a dynamic avatar, which is functionally equivalent to a digital axiograph. This enables the virtual articulator to be programmed individually for each patient.

Recording both tooth-guided and muscle-guided mandibular movements enabled the design of a physiologic occlusion adapted to the patient’s true functional envelope. In this case, mandibular trajectories captured during mastication (using a cotton pellet) were digitally processed to guide the morphology of functional surfaces, ensuring precise posterior dental disocclusion and accurate replication of the patient’s anterior guidance dynamics.
Phase 2: Digital Design and Clinical Validation
In the space of a day following the preliminary consultation, the project encompassing the digital prosthesis was presented in its entirety the patient. The fabrication of a mock-up was facilitated by a 3D-printed model during the same session. The validation of the esthetic and functional parameters was conducted intraorally, and the results were immediately approved.The mock-up functioned as the template for both diiode laser gingivoplasty and for the tooth preparations. Provisional restorations for both arches were fabricated and placed in order to validate aesthetic, occlusal, and functional parameters during the temporization phase.



The rehabilitation process was initiated with the mandibular arch, thus enabling the refinement of the maxillary palatal contours against the mandibular ceramics. Following validation, definitive maxillary crowns were fabricated without altering the previously approved palatal profiles.
An intraoral “situation scan” of the temporary crowns was recorded using Aoralscan 3® to preserve the validated parameters. Segmenting the maxillary rehabilitation was adopted as a preventative measure for bruxing patients, enhancing long-term prognosis.
The patient and clinical team reported a high level of satisfaction with the aesthetic and functional outcomes



Discussion
Anterior guidance is defined as the dynamic relationship between the maxillary and mandibular anterior teeth during functional movements. The configuration of the upper anterior dentition is principally determined by the palatal surfaces of the maxillary incisors and canines, incorporating parameters such as overjet, overbite, incisal inclination, and canine guidance.
A functional anterior guidance system ensures complete and immediate posterior disocclusion during mandibular excursions, thereby preventing occlusal interferences. Conversely, an absence of guidance can result in posterior interferences and parafunctional stress.
Posterior tooth morphology—specifically the parameters of cusp height and inclination—is found to be directly influenced by the parameters of anterior guidance. For instance, a steeper condylar path permits longer cusps and deeper fossae without interference.
Condylar guidance, signifying the movement trajectory of the condyle-disc complex within the glenoid fossa, is ordinarily delineated by the sagittal condylar inclination and the Bennett angle. Hanau’s Quint postulates that masticatory harmony arises from the interrelationship among condylar guidance, incisal guidance, compensating curves, occlusal plane inclination, and cusp height. Each of these is shown to require compensatory adjustment when another is altered.
Nevertheless, the relationship between anterior and condylar guidance remains a subject of depth. One school of thought asserts that incisal inclination is not contingent on TMJ morphology. This school emphasises that anterior guidance should be reconstructed according to both aesthetic and functional criteria while ensuring posterior disocclusion. In contrast, the functionalist school of thought posits a correlation between condylar morphology and incisal slope, proposing a reconstructed incisal guidance that is approximately 10° steeper than the condylar inclination. This approach is purported to enhance anterior control of mandibular movements.
Modern prosthodontics has undergone a shift towards the adoption of individualised, patient-specific approaches. Digital technologies such as METISMILE® facilitate precise transfer of recorded mandibular kinematics to virtual articulators, thus reducing reliance on average values.
Cone-Beam Computed Tomography (CBCT) is considered the reference standard for TMJ anatomical assessment and quantification of condylar inclination, while digital axiography complements it by enabling real-time motion analysis. The selection of the reference plane (axio-orbital, Frankfurt, or Camper) has been demonstrated to exert a significant influence on the measured values; consequently, standardisation is imperative for the assurance of reproducibility.
Conclusion
Recent advancements in digital technology have rendered it feasible to incorporate occlusal rehabilitation into a comprehensive CAD/CAM workflow, encompassing intraoral scanning, dynamic motion recording, virtual design and definitive manufacturing. The METISMILE® system is a prime example of this evolution, as it integrates aesthetic, functional and physiological precision. The employment of bespoke digital methodologies engenders prostheses that not only restore physical appearance, but also align with the patient’s authentic functional dynamics, thereby ensuring prolonged stability and comfort.
Share this on social media: